This policy provides guidance and resources for providing services to lesbian, gay, bisexual, transgender, queer, questioning (LGBTQ+) children/nonminor dependents (NMDs) and information on placement requirements for Transgender and gender non-conforming (TGNC) children/NMDs in out-of-home care based on current legislation and best practice.
This policy guide was updated from the 02/28/2020 version to reflect policy and protocol updates based on Assembly Bills (ABs) 959 and 175 regarding the Foster Youth Bill of Rights; All County Letter (ACL) 21-149 regarding the documentation of Sexual Orientation, Gender Identity and Expression (SOGIE); and to include information regarding the LGBTQ+ Tailored Services to Youth program.
POLICY
In a 2014 study conducted by the RISE Program of the Los Angeles LGBT Center, the Williams Institute at UCLA, and Holarchy Consulting, findings showed that:
19% of foster youth sampled in Los Angeles County identify as LGBTQ. Meaning that there are between 1.5 and 2 times more LGBTQ+ youth as a percentage of young people in foster care than outside foster care.
94% of the youth sampled were youth of color, indicating that many of them likely faced both racial and anti-LGBTQ discrimination.
5.6% of the foster youth sampled identified as transgender, a significant overrepresentation compared to an estimated .3 % of the national population.
Not only are LGBTQ+ youth overrepresented in the foster care population, there are also significant disparities in experience between LGBTQ+ youth and their non-LGBTQ+ counterparts. According to the Williams-Holarchy study LGBTQ+ children/NMD:
Report worse experiences in the foster care system compared to non-LGBTQ+ children/NMD;
Have a higher than average number of foster care placements;
Are more likely to live in a group home;
Are more likely to have been hospitalized for emotional reasons; and
Are more likely to experience homelessness at some point in their lives
Sexual Orientation, Gender Identity, and Expression (SOGIE)
LGBTQ+ children/NMDs have the right to be free of harassment and discrimination based on their actual or perceived SOGIE (sexual orientation, gender identity, or gender expression), or association.
LGBTQ+ children/NMDs shall not be exposed to attempts to change their SOGIE and cannot be forced to hide their SOGIE in order to get support, receive services, be placed, etc.
Confidentiality
Any information about a child/NMD’s sexual orientation, gender identity and expression, including LGBTQ+, however the information is obtained is to be treated as private and confidential. As indicated in All County Letter 21-149, all information regarding a child/NMD’s SOGIE is confidential and not to be disclosed to anyone or documented without the child/NMD’s expressed consent or otherwise as authorized/required by law. Unwarranted disclosure of SOGIE information may subject a child/NMD to rejection, ridicule, harassment, or abuse. Caution should be taken when recording or sharing this information and should only be done when necessary to advance the child/NMD's well-being and after consulting with the child/NMD, after explaining their confidentiality rights and securing the child/NMD's written consent. The child/NMD may withdraw their consent or limit it at any time.
Information about a child/NMD's identification as LGBTQ+ should not be disclosed to other children/NMDs, outside parties, individuals, or agencies, including health care or social service providers, without the child/NMD's permission/consent, unless such disclosure is necessary to comply with state or federal law or relevant to an emergency mental health or medical incident.
The extent and limits of keeping confidential information about a child/NMD's SOGIE is to be explained to the child/NMD. If for any reason disclosure of the information is required to be shared with another individual, the child/NMD is to be informed to whom the information will be disclosed and the reason for the disclosure. In such a case, the individual receiving the information is to be informed about the parameters of said disclosure and the party disclosing the information needs to plan to mitigate any risks pertaining to the disclosure.
Additionally, per ACL 21-149, child welfare social workers and juvenile probation officers (SWs/POs) should explain confidentiality and the limits of confidentiality in a way that is age and developmentally appropriate and be open and honest from the beginning of asking any SOGIE questions. Children and NMDs are more likely to share private information about their SOGIE when they feel supported and know what to expect. When discussing limits of confidentiality with a child or NMD, the SW/PO should explain to them that they have the right to keep their SOGIE information private and they can authorize or deny to whom their SOGIE information is disclosed. However, they should also clarify for the child/NMD that there are some circumstances in which their information will be required to be shared even without the child’s/NMD’s consent.
Different scenarios may arise on a case-by-case basis regarding LGBTQ+ children/NMDs. For any concerns related to confidentiality prior to the disclosure of SOGIE information, CSWs and SCSWs may conference and/or consult with County Counsel.
Medical Records
The disclosure of medical and mental health information, including Protected Health Information (PHI) is regulated by federal and state laws. Under federal law, the Health Insurance Portability and Accountability Act (HIPAA) of 1996, protects the privacy of patient health information. HIPPA limits disclosure of what it calls "protected health information" (PHI). Under state law, California Code 56, et seq, protects medical and mental health information. Pursuant to federal and state laws, DCFS staff may not disclose medical or mental health information unless a specific legal exception applies. Unauthorized disclosure of confidential medical or mental health information carries both civil and criminal penalties.
Court Reports
A child/NMD’s sexual orientation and gender identity is confidential and is not to be disclosed in any court reports unless, after being advised of their confidentiality rights and discussing the possible disclosure and who will receive the information, the child/NMD has given permission to share the information.
Disclosures to Family/Resource Parents
DCFS staff shall not disclose information about a child/NMD's status as LGBT+ to a child/NMD's parent, legal guardians, resource parents, or other family members without the informed and expressed consent of the child/NMD including in CFTMs.
Regardless of a parent/s wishes for disclosure it is the child/NMD’s right to choose whether or not to disclose their sexual orientation.
Case Planning and the Child and Family Team (CFT)
Affirming behaviors from parents/resource parents of the child/NMD's SOGIE may vary and can be a fluid process. The Child and Family Team (CFT) will work to protect the child/NMD from potential rejecting experiences in their living situation, and in service provision including but not limited to: educational, medical, mental health environments; and extracurricular activities. A goal of the case planning process is to be affirming of the child/NMD, as well as their peers, and parents/resource parents wherever they may be in their own process. Therefore, the child/NMD’s SOGIE shall be a consideration in all case planning processes. A subject-matter expert, with demonstrated competency, may be retained to support this process, if necessary. In addition, the expert may be involved in CFTMs with the child/NMD’s permission. This includes but is not limited to office-designated LGBTQ+ champions and external stakeholders/providers.
The CFT will drive the case planning process and ensure that significant connections are included in the plan for the child/NMD. The CFT will ensure that parents/resource parents have sufficient services, support, and resources to meet the needs of the child/NMD in their care. The CFT will assist with accessing these supportive services and resources. In addition, it will provide and facilitate whatever additional expertise is necessary to form and/or maintain healthy relationships between parents/resource parents and children/NMDs, including advocacy and education of outside parties (e.g. educational, legal, medical).
Per Senate Bill (SB) 731, children/NMDs have the right to be placed in homes and facilities according to their gender identity, regardless of their sex assigned at birth or sex/gender marker listed in their court, child welfare, medical, or vital records.
Self-identification is a fluid process, which may occur before, during, or after being placed. While children/NMDs have the right to be placed according to their gender identity, not all LGBTQ+, transgender and/or gender non-conforming (TGNC) children/NMDs will want to be placed based on their gender identity; however, some children/NMDs will be clear in their desire and must be placed accordingly. As per legislation, the intake process must include assessment of all the child/NMD’s placement needs, including but not limited to the child/NMD's gender identity.
A child/NMD’s SOGIE identity is confidential information. Staff may not divulge this information to anyone, including a child/NMD's roommate, without the child/NMD's expressed consent to document and/or disclose.
A child’s/NMD's gender identity should not be the only deciding factor when considering room assignments. Roommate compatibility is to be discussed during ongoing contact with the child/NMD. As per Contact Requirements and Exceptions, the purpose of the social worker's contact with the child is to assess the safety and well-being of the child and to achieve the following:
Monitor the child’s physical, emotional, social and educational development, and their mental/behavioral health needs.
Assist the child in preserving and maintaining their culture, this includes religious and ethnic identity and sexual orientation, gender identity, and expression (SOGIE).
Staff placing a child/NMD should advocate for rooming assignments based on the needs of the child/NMD. Placement decisions are to be made in the best interest of the child/NMD based on recommendations from the CFT, Transitional Shelter Care (TSC) Program, Resource Family Approval (RFA) CSW, Multi-Disciplinary Team (MDT), and the child/NMD.
Gender-affirming Health Care
Per AB 2119children/NMDs in foster care have the right to receive gender-affirming medical and mental health care services and are to be involved in the development of case plan elements related to placement and gender-affirming health care, consistent with their gender identity.
Reproductive Health
Per state law, children/NMDs in foster care are entitled to being informed about their reproductive and sexual health care rights, upon entry into foster care and at least once every six months at the time of a regularly scheduled contact. CSWs should also ensure that children/NMDs have access to reproductive health care and assist with removing any barriers to care. Refer to the Youth Reproductive Health and Pregnancy 0600-507.10 policy.
All DCFS staff shall establish and maintain a culture of safety, inclusivity, and dignity where every child/NMD’s identity is affirmed and their well-being is ensured.
Sexual Orientation, Gender Identity, and Expression (SOGIE)
The sharing of SOGIE information by the child/NMD is voluntary and the child/NMD may decline to disclose any of their SOGIE information.
Example 1
If consent is given by the child/NMD, document in CWS/CMS what the child/NMD consents to. Also, update the information if changes are reported by the child/NMD. The CSW should inform the child/NMD of instances when their SOGIE may need to be shared with other professionals, letting the child/NMD know specifically how this information will be used and by which legally authorized individual.
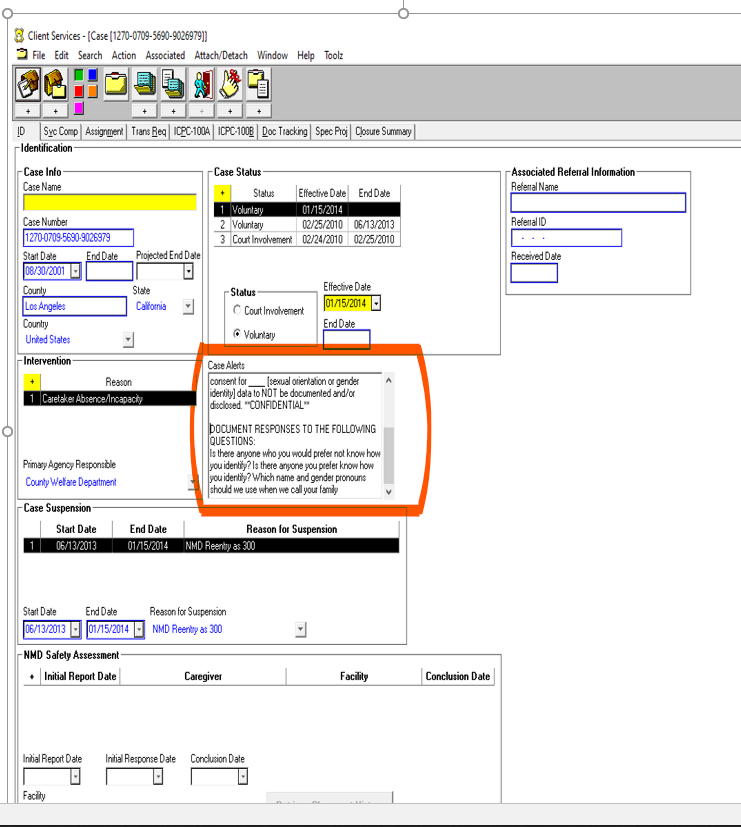
The CSW should clarify in advance with whom it is acceptable to share the information, including when the child/NMD is being referred to other resources for support. If the child/NMD has identified specific people with whom the information should not be shared, make sure that it is clear to all staff and is documented in the CWS/CMS Client ID Tab inside the Case Alerts box (See Example 2 below).
Example 2
Subjective opinions or assumptions on a child/NMD’s SOGIE should neither be made nor documented in CWS/CMS.
There is no right or wrong age to ask a child/NMD about their sexual orientation and gender identity and expression.
Engage children/NMDs who are developmentally and cognitively capable of understanding and discussing gender, in an age-appropriate discussion of their preferred gender expression and the gender with which they identify.
A child’s/NMD’s SOGIE is not static and may change during the duration of a case.
During ongoing contact with the child/NMD, CSWs are to have age-appropriate conversations regarding a child/NMD’s SOGIE and are to update consent in CWS/CMS accordingly.
Per WIC 827, a child’s/NMD’s SOGIE is not to be disclosed to other individuals or agencies, without the child’s/NMD’s informed and express consent.
Refer to the glossary of SOGIE data frame definitions to ensure consistent usage and unified understanding of SOGIE terms.
Ensure that CSWs utilize best practices when inquiring about SOGIE and, if applicable, appropriately documented the response provided in the CWS/CMS Client Notebook ID page in the Sexual Orientation, Gender Identity, and Gender Expression fields.
Ensure that confidentiality is followed in court reports and that SOGIE is only disclosed if a child/NMD has provided informed and express consent.
Confidentiality
CSW Responsibilities
As indicated in All County Letter 21-149, all information regarding a child’s/NMD’s SOGIE is confidential and not to be disclosed to anyone or documented without the child’s/NMD’s informed and express consent or unless otherwise authorized/required by law.
The CSW should ask the child/NMD the following questions; Is there anyone whom you would prefer not know how you identify? Is there anyone you prefer to know how you identify? Which name and gender pronouns should we use when we call your family? Responses to these questions are to be documented in the CWS/CMS Client ID page in the Case Alerts Box: (Refer to Example 2 above.)
Each category of SOGIE data shall only be documented if a child/NMD provides informed and express consent to document and disclose. For any field(s) a child/NMD does not provide informed and express consent, the CSW shall only select “Declines to state” in CWS/CMS and should not otherwise document and/or disclose.
Documenting Consent
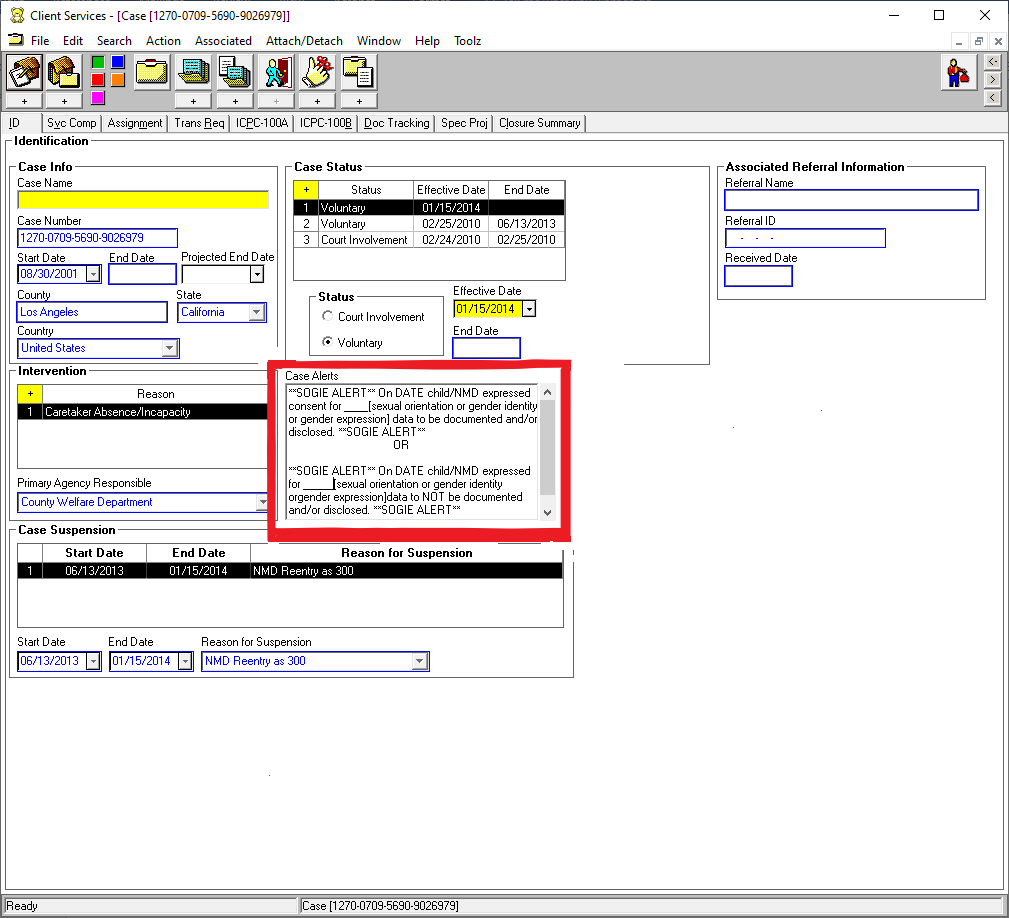
If a child/NMD expresses consent for SOGIE to be or NOT be documented and/or disclosed, the CSW is to document in the CWS/CMS Case ID Page in the Case Alerts Text Box the following (See Example 3):
**SOGIE ALERT** On DATE child/NMD expressed consent for ____ [sexual orientation or gender identity or gender expression] data to be documented and/or disclosed. **SOGIE ALERT**
Or
**SOGIE ALERT** On DATE child/NMD expressed for ____ [sexual orientation or gender identity or gender expression] data to NOT be documented and/or disclosed. **SOGIE ALERT**
Example 3
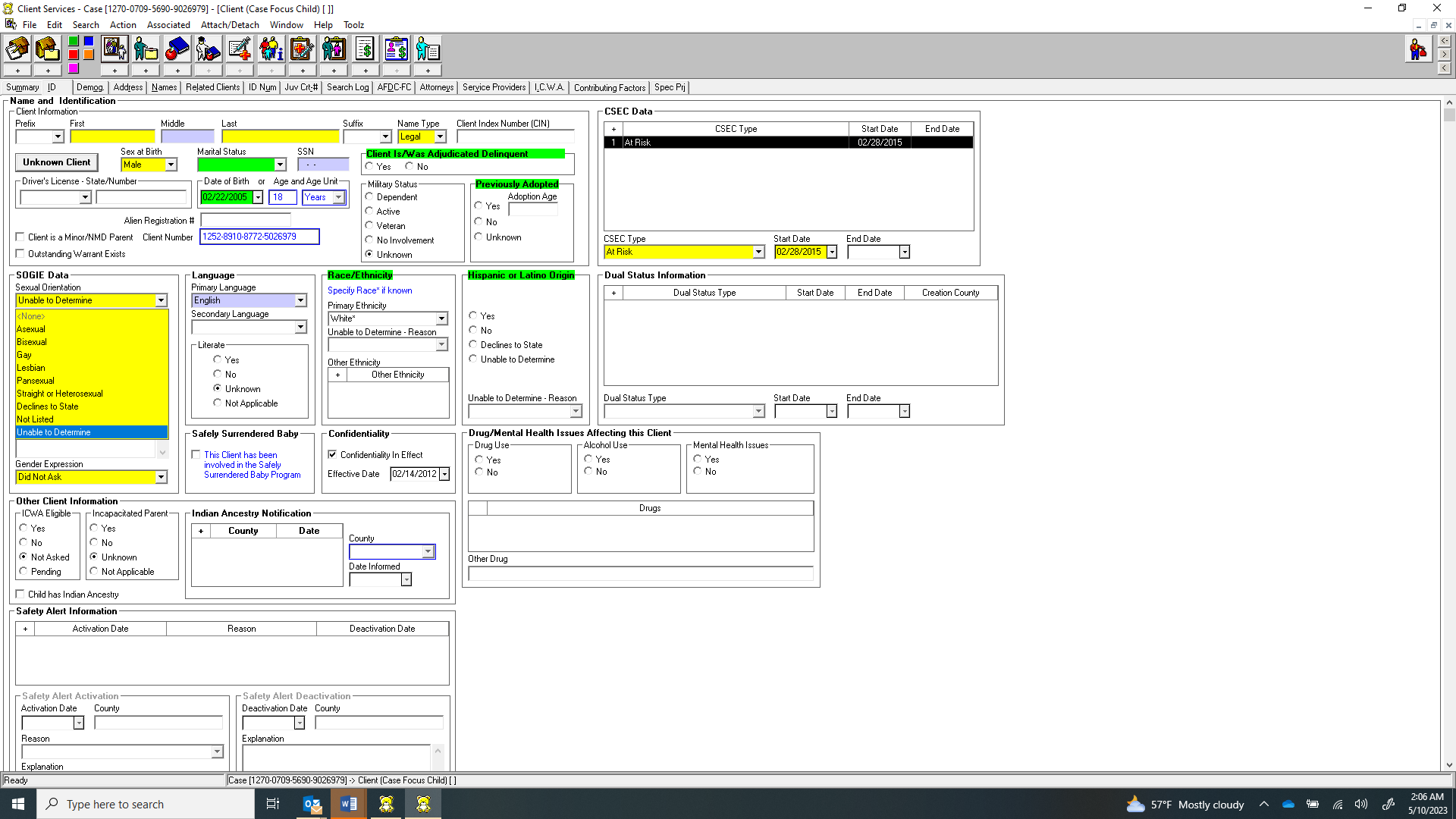
If a child/NMD expresses consent for SOGIE to be documented and/or disclosed, the CSW is to select the corresponding choices from the SOGIE drop down menus (See Examples 4 and 5 below)
Example 4
Example 5
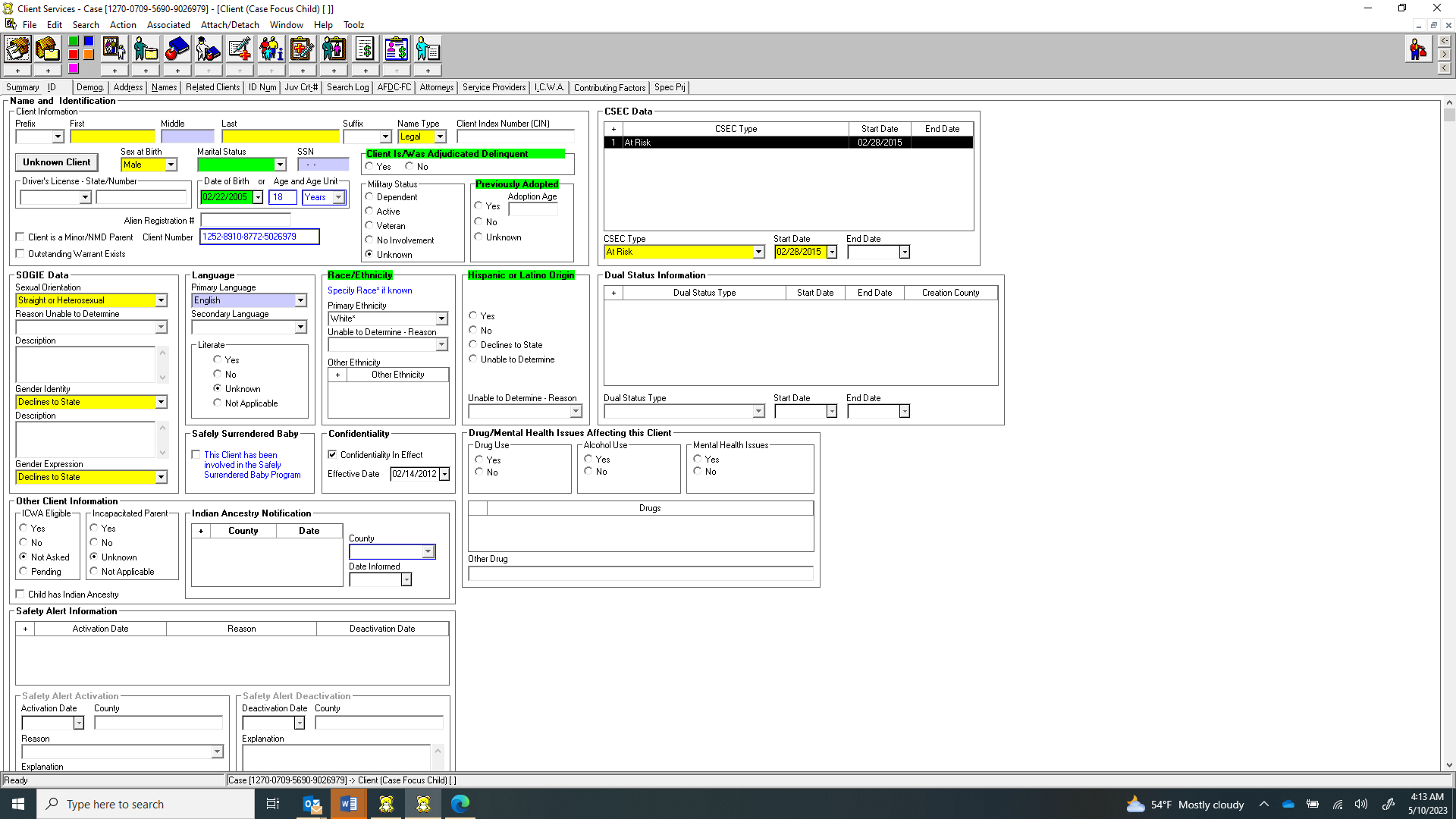
If a child/NMD discloses that they are heterosexual (sexual orientation), gender queer (gender identity), and feminine (gender expression); however, express that they do not give consent for their gender identity or expression to be documented or disclosed the CSW shall only document the sexual orientation as disclosed in the Sexual Orientation field, and in the Gender Identity and Gender Expression fields, the CSW shall select “Declines to State.” (See Example 6 below)
Example 6
In the CWS/CMS Case ID page in the Case Alerts text box the CSW is to include the following (See prior Example 3):
** SOGIE ALERT ** On DATE child/NMD expressed consent for sexual orientation to be documented ** SOGIE ALERT**
Placements
CSWs may not document or disclose SOGIE information to anyone, including a child/NMD's roommate(s), parents/guardians, or resource parents without the child/NMD's expressed consent to do so. Staff should advocate for rooming assignments based on the needs of the child/NMD.
All placements shall be safe and affirming of children/NMD’s SOGIE and placement decisions are to be made in the best interest of the child/NMD based on recommendations from the CFT, Transitional Shelter Care (TSC) Program, Resource Family Approval (RFA) CSW, MDT, and the child/NMD.
To help ensure that all placements are safe and affirming of a child/NMD’s SOGIE, the following should be discussed with a transgender youth/NMD when considering placements:
A transgender child/NMD should be asked if their gender identity may be disclosed and/or if the fact that they are transgender may be disclosed to intake workers, caretakers, etc.
If a transgender child/NMD does not consent to their gender identity being disclosed, they should be advised that the gender assigned to them at birth will be disclosed to intake workers, caretakers, etc.
At no time should a child/NMD’s identification as transgender be disclosed without their explicit consent; while, as default, a child/NMD’s gender assigned at birth will be disclosed unless the child/NMD gives explicit consent to disclose their gender identity
For additional assistance with finding placements, CSWs may refer to the Transitional Shelter Care
The disclosure of medical and mental health information, including Protected Health Information
(PHI) is regulated by federal and state laws. Under federal law, the Health Insurance Portability and Accountability Act (HIPAA) of 1996, protects the privacy of patient health information. This includes but is not limited to gender affirming care. CSWs may refer to the Health and Medical Information 0600-500.20 policy.
Court Reports
SOGIE information is not to be documented in Court Reports or otherwise disclosed in court proceedings unless a child/NMD has expressed consent for said information to be documented and/or disclosed. In such a case, the CSW shall follow the documenting consent protocol.
Disclosures to Parents/Guardians and Resource Parents
Per WIC 827, a child’s/NMD’s SOGIE is not to be disclosed to other individuals or agencies, without the child/NMD’s permission. Staff is not to disclose or document a child’s/NMD’s SOGIE to a child’s/NMD’s parents/guardians and resource parents without the child/NMD’s expressed consent to do so. In such a case, the CSW shall follow the documenting consent protocol.
Regardless of a parent’s wishes for disclosure it is the child’s/NMD’s right to choose whether or not to disclose their sexual orientation
Case Planning and the Child and Family Team (CFT)
A child/NMD’s CFT shall establish and maintain a safe and inclusive culture where the child/NMD’s SOGIE is affirmed and their well-being is ensured.
CSW Responsibilities
CSWs are to ensure that a child/NMD’s SOGIE consent is confirmed prior to every CFTM as it pertains to any parties who may be present. Documenting consent protocol shall be followed to reflect any updates and CSWs shall follow all procedures for Child and Family Team meetings. Refer to the Child and Family Teams 0070-548.01 policy for further guidance.
Transgender and Gender Non-Conforming (TGNC) Children/NMDs
According to SB731TGNC children/NMDs have the right to be placed according to their gender identity, irrespective of the sex/gender marker listed on any legal/medical documents. Information regardingSB 731 (2015), shall be provided to all children/NMDs prior to out of home placement, parents/guardians at time of removal, and resource parents at orientation and redetermination.
When shared accommodations are required, DCFS shall discuss roommate compatibility to ensure that assigned roommates are affirming of the child/NMD. TGNC children/NMDs should be actively engaged in the placement process and be given specific options, so that they can help identify the situations that will work best for their needs and safety.
Placements
Bathroom/Shower Use
TGNC children/NMDs have the right to access bathrooms and showers that align with their gender identity, regardless of sex assigned at birth and/or legal documentation. Safety planning and prudent parenting standards shall be utilized for TGNC children/NMDs regarding the use of bathrooms and showers. Alternative arrangements should only be made at the request of the TGNC child/NMD; TGNC children/NMDs shall not be compelled to use alternative bathrooms/showers. Prudent Parenting standards should apply when the child's/NMD's needs may put them in danger. Alternative arrangements may include, but are not limited to:
Accessibility of single stall, gender neutral bathrooms, and/or private showers;
Staff supervision during use of communal bathrooms/showers; and
A separate shower schedule for TGNC children/NMDs if they request it.
Access to Services/Programs
TGNC children/NMDs have the right to participate in and have access to all available services/programs. Resource parents and service providers are to provide care and support inclusive of their identity. The CFT can be utilized to access additional resources (e.g., gender affirming care, programs, etc.) with expressed consent from and at the request of the child/NMD.
Beginning March 1, 2022, children, youth and young adults who identify as LGBTQ+ can voluntarily participate in the LGBTQ+ Tailored Services to Youth program. The program is an opportunity for LGBTQ+ youth to receive necessary and beneficial services, inclusive of and while celebrating their SOGIE. To access the program, the youth needs to be referred by electronic submission. More information, including the referral form, can be found at https://dcfs.lacounty.gov/youth/lgbtq-youth/. Once a youth self-identifies as LGBTQ+, and consent is received, CSWs should provide the LGBTQ+ Tailored Services to Youth program information to the youth and ask if youth would like to participate. If the youth agrees, the CSW should submit a referral as instructed and according to referral form.
Name and Use of Pronouns
TGNC children/NMDs may designate a name and pronouns to be used that reflects their identity, even if their name has not been legally changed and/or legal documentation has not been updated. Placements shall address TGNC children/NMDs using their asserted name and pronouns. DCFS shall ensure that all placements are in compliance with legal requirements, are affirming, and utilize best practices. A TGNC child’s/NMD's personal rights must be respected; misgendering and use of derogatory terms by any party shall be addressed and may be considered maltreatment.
A TGNC child's/NMD's asserted name and pronouns shall be included on all documents in conformity with confidentiality practices. Using the child’s/NMD’s asserted name and/or pronouns shall only be done with the expressed consent of the child/NMD and to the extent the child/NMD has given their consent. On all DCFS and court documents, the child/NMD will first be referred to by their legal name, along with the child's/NMD's asserted name as an “also known as” (AKA), with the asserted name and pronouns emphasized in order to minimize confusion as to which name/pronouns to use. Thereafter, the child/NMD shall be referred to by their asserted name and pronouns.
EXAMPLE:
Jane Doe, AKA John Doe (they/them/theirs), is currently placed with their paternal aunt. They are attending their school of origin where........
In the event that the child/NMD expresses an interest in changing their legal name and/or gender marker, petitions to the court may be utilized. CSWs shall consult with minor’s counsel on this process if the child/NMD consents and the CSW can refer children/NMDs to the Los Angeles Superior Court’s self-help page at https://www.courts.ca.gov/41237.htm for further information. DCFS will not/cannot petition for any legal name change, but can make the juvenile court aware if this is something the child/NMD desires and the child/NMD has given consent to bring this to the court’s and/or minor’s counsel’s attention.
Gender-Affirming Health Care
“Gender-affirming health care” is defined in WIC 16010.2 as medically necessary health care that respects the gender identity of the patient, as experienced and defined by the patient, and may include, but is not limited to, the following:
Interventions to suppress the development of endogenous secondary sex characteristics.
Interventions to align the patient’s appearance or physical body with the patient’s gender identity.
Interventions to alleviate symptoms of clinically significant distress resulting from gender dysphoria, as defined in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
Gender identity formation is a typical, healthy part of child development and generally begins around two (2) years old. However, healthy development may be impacted by negative bias and rejection. When a child/NMD expresses an incongruence with regards to their gender identity as it relates to their sex assigned at birth, qualified and affirming experts may be consulted, and age-appropriate resources shall be provided to the child/NMD.
When possible and appropriate, parents/guardians should be involved in the child's/NMD's health care. Children/NMDs can receive hormone therapy, including but not limited to: hormone blockers and hormone replacement therapy; however, parental or court consent is required, with limited exceptions (Family Code 6922). Should the child/NMD request any gender affirming care, the agency shall have the child/NMD assessed by a qualified, licensed, and affirming medical practitioner with competency in working with transgender children/NMDs as soon as possible.
If any child/NMD placed is already in the process of transitioning through the use of hormones, DCFS may need legal approval (parental or court) for continued treatment and must obtain medical advice, guidance, and clearance for formal prescriptions; which must be obtained promptly to ensure continuity of care. DCFS shall ensure that staff and resource parents are in compliance with medical protocols and the physician’s treatment plan. In cases where the child/NMD has an anticipated change of placement, a healthcare continuity plan shall be developed.
In the event that the child/NMD expresses the desire for gender-affirming care and/or the medical professional recommends gender-affirming care, but consent is not given by the medical rights holder, a court hearing date shall immediately be requested to approve said care.
Reproductive Health (SB89)
For children age ten (10) and older, the CSW shall be responsible for ensuring that children/NMDs receive age-appropriate, medically accurate, culturally sensitive sexual and reproductive health information that includes:
Informing children/NMDs that they may access age-appropriate, medically accurate information about reproductive and sexual health care, including, but not limited to, unplanned pregnancy prevention, abstinence, use of birth control, abortion, and the prevention and treatment of sexually transmitted infections. Refer to Foster Youth Bill of Rights for further information.
Informing children/NMD, in an age and developmentally appropriate manner, of their right to consent to sexual and reproductive health services.
Informing children/NMDs about their confidentiality rights regarding medical services and seeking the child’s/NMD's written consent prior to any disclosure of their sexual or reproductive health information. Also, informing children/NMDs of their right to withhold consent to such disclosure(s).
Informing the children/NMDs how to access reproductive and sexual health care services and facilitated access to that care, including by assisting with any identified barriers to care, as needed.
A copy of the Foster Youth Bill of Rights upon entry into foster care and at least once every six (6) months at the time of scheduled contact.
The right to fair and equal access to all available services, placement, care, treatment and benefits, and to not be subjected to discrimination or harassment based on actual or perceived race, ethnic group identification, ancestry, national origin, color, religion, sex, sexual orientation, gender identity, mental or physical disability, or Human Immunodeficiency Virus (HIV) status.
Different scenarios may arise on a case-by-case basis regarding LGBTQ+ children/NMDs. CSWs and SCSWs are to conference and/or contact County Counsel for any questions.
All County Letter 17-64 – Outlines the placement changes for children and NMDs per Senate Bill 731 (2015). It requires that children and NMDs in out of home care shall be placed according to their gender identity if the child/NMD so desires per WIC 16006, WIC 16001.9(a)(24), H&S Code 1502.8.
All County Letter 16-82 – Outlines the reproductive and sexual health care and related rights of youth and Nonminor Dependents (NMDs) in foster care.
All County Letter 19-27 –Gender Affirming Care for Minor and Nonminor Dependents in Foster Care.
All County Letter 21-149 – Documentation of Sexual Orientation, Gender Identity and Expression Information in the Child Welfare Services/Case Management System.
AB959- Lesbian, Gay, Bisexual and Transgender Disparities Reduction Act
AB 2119- Gender Affirming Care for Minor and Nonminor Dependents in Foster Care
SB 731(2015)- Requires children and nonminor dependents in an out-of-home placement to be placed according to their gender identity, regardless of the gender or sex listed in their court or child welfare records.
Health and Safety Code section 1502.8 – Requires the Department of Social Services to adopt regulations consistent with the new personal right of minors and NMDs in foster care to be placed in out-of-home care according to their gender identity, regardless of the gender or sex listed in their court or child welfare records.
Welfare and Institutions Code section 16001.9(a)(24) – Affords the right of all minors and nonminors in foster care to be placed in out-of-home care according to their gender identity, regardless of the gender or sex listed their court or child welfare records.
Welfare and Institutions Code section 16006 – Requires that all children and NMDs in out-of-home care be placed according to their gender identity, regardless of the gender or sex listed in their court or child welfare records.
Title 22, Division 6, Chapter 9.5, Section 89377 – States that a caregiver is responsible for applying the Reasonable and Prudent Parent Standard and what factors to consider.
A non-specific file number generated by the Emergency Response Command Post (ERCP) identifying a placement case that is transferred from ERCP directly to a regional Family Maintenance and Reunification (FM&R) or generic (G) file.
Los Angeles County Department of Mental Health's (DMH) 24 hour, 7 (seven) day a week hotline: Emergency psychiatric services are coordinated through ACCESS. ACCESS offers information regarding all types of mental health services available in Los Angeles County. CSWs may request a joint response with FRO by contacting ACCESS at (800) 854-7771.
The term includes physical injury or death inflicted upon a child by another person by other than accidental means, sexual abuse as defined in Section 11165.1, neglect as defined in Section 11165.2, unlawful corporal punishment or injury as defined in Section 11165.4, or the willful harming or injuring of a child or the endangering of the person or health of a child, as defined in Section 11165.3, where the person responsible for the child's welfare is a licensee, administrator, or employee of any facility licensed to care for children, or an administrator or employee of a public or private school or other institution or agency. 'Abuse or neglect in out-of-home care' does not include an injury caused by reasonable and necessary force used by a peace officer acting within the course and scope of his or her employment as a peace officer.
The team is made up of former RUM (Resource Utilization Management) staff who have experience in finding placement for high risk/needs children. APT Specialist CSWs can assist Regional CSWs expedite the process in finding placement/replacement after hours and/or when all other efforts have been unsuccessful.
Renamed to Centralized Placement Program (CPP)
Active investigation means the activities of an agency in response to a report of known or suspected child abuse. For purposes of reporting information to the Child Abuse Central Index, the activities shall include, at a minimum: assessing the nature and seriousness of the known or suspected abuse; conducting interviews of the victim(s) and any known suspect(s) and witness(es) when appropriate and/or available; gathering and preserving evidence; determining whether the incident is substantiated, inconclusive, or unfounded; and preparing a report that will be retained in the files of the investigating agency.
A mandatory statewide program that provides financial support to families in order to facilitate the adoption of children who would otherwise be in long-term foster care. The intent of this program is to remove limited financial resources as a barrier to adoption.
State licensed adoption practitioners who are authorized to help the adopting family in obtaining consents from birth parents in non-relative independent adoption.
An order/decision which is contrary to a DCFS recommendation and which DCFS believes, if carried out, will jeopardize the safety of a child; and an order/decision which adversely affects the administrative and/or operational functioning of DCFS. This includes, but is not limited to, orders, which are contrary to DCFS policy and/or state or federal regulations; and/or, penalizes DCFS for the actions or inaction of a CSW and/or DCFS.
CSW is requesting a ruling on the warrant on a weekend, holiday, or during non-court hours. (Same as expedited but the matter cannot wait until the next court day for a ruling.)
The adoption of a child in which DCFS is a party to or joins in the petition for adoption. DCFS has custody of the child and approved the applicant assessment (adoption home study).
Foster care financial assistance paid on behalf of children in out-of-home placement who meet the eligibility requirements specified in applicable state and federal regulations and laws. The program is administered by DCFS.
An identified or unidentified man who: could be or claims to be the father of the child; or is claimed by the birth mother to be the child’s father; or is identified on the child’s birth certificate prior to January 1, 1997 and does not meet the definition of a presumed father.
Benefits equal to the rate that a Regional Center vendorized home receives for a child that requires the same level of care. These rates are established by the California Department of Development Services and only available for the foster care and Adoption Assistance Benefits (AAP) set prior to the establishment of the dual agency rate.
A hearing in which the court has ordered all affiliated parties to appear to address a matter before the court.
Appellate review refers to the power of a higher court to examine the decision or order of a lower court for errors. Appellate procedure consists of the rules and practices by which appellate courts review trial court judgments. Appellate review performs several functions, including: the correction of errors committed by the trial court, development of the law and precedent to be followed and anticipated in future disputes, and the pursuit of justice.
This is the term used for an agency adoption to determine AAP eligibility.
An assessment usually conducted by a child welfare of adoption agency of the suitability of a prospective adopting family prior to an adoptive placement.
A motion for rehearing or reconsideration seeking to alter or amend a judgment or order.
A family participating in DPSS CalWORKs
When a report has been made about a child alleging abuse and/or neglect and the child's sibling(s) are also at risk of abuse and/or neglect.
A foster parent, relative or nonrelative extended family member (NREFM) who has applied to adopt the child residing in his or her care. S/he is considered to be "attached" to the child because of an existing relationship.
Disease-carrying microorganisms that may be present in human blood. These pathogens include, but are not limited to, hepatitis B and C virus (HBV and HCV) and human immunodeficiency virus (HIV). Depending on the disease, they may be transmitted by direct skin contact to blood, semen, and vaginal secretions. Feces, urine, vomit, sputum, and nasal secretions may be infectious only if they also contain blood.
A redeemable certificate used as a substitute for currency. Transit companies other than the Metropolitan Transit Authority (MTA) issue bus passes.
A permit or authorization to ride at will, without charge. Passes are valid for the current month. Transit companies other than the MTA issue bus passes.
A piece of metal used as a substitute for currency.
California's food stamp program
California Statewide Automated Welfare System. The California Statewide Automated Welfare System (CalSAWS) Project and Consortium is the automated welfare business process in California which has served all 58 California counties since 2023. The implementation of CalSAWS merged California’s most recent three (3) county-level consortia welfare systems and supports six (6) core programs: California Work Opportunity and Responsibility to Kids (CalWORKs), Supplemental Nutritional Assistance Program (SNAP) known as CalFresh in California, Medi-Cal, Foster Care, Refugee Assistance, and County Medical Services. It encompasses the following functions: eligibility determination, benefit computation, benefit delivery, case management and information management. CalSAWS replaced the LEADER Replacement System (LRS), which had replaced LEADER (Los Angeles Eligibility, Automated Determination, Evaluation, and Reporting) and sixteen (16) other legacy systems in 2016.
A system to determine if the subject of an inquiry by DCFS, law enforcement, the District Attorney or any other appropriate inquiring agency possesses a criminal record. DCFS may only request a CLETS clearance when related to child protective services issues.
California Regional Centers are nonprofit private corporations that contract with the State Department of Developmental Services (DDS) to provide or coordinate services and supports for individuals with developmental disabilities.
CalWORKs is a welfare program that gives cash aid and services to eligible needy California families. The program serves all 58 counties in the state and is operated locally by county welfare departments. If a family has little or no cash and needs housing, food, utilities, clothing or medical care, they may be eligible to receive immediate short-term help. Families that apply and qualify for ongoing assistance receive money each month to help pay for housing, food and other necessary expenses.
The child's parent has been incarcerated, hospitalized or institutionalized and cannot arrange for the care of the child; parent's whereabouts are unknown or the custodian with whom the child has been left is unable or unwilling to provide care and support for the child.
Parent or guardian's mental illness, developmental disability or substance abuse. The child's parent or guardian is unable to provide adequate care for the child due to the.
The team is made up of former RUM (Resource Utilization Management) staff who have experience in finding placement for high risk/needs children. APT Specialist CSWs can assist Regional CSWs expedite the process in finding placement/replacement after hours and/or when all other efforts have been unsuccessful.
Previously known as the Accelerated Placement Team (APT).
The non-accidental commission of injuries against a person. In the case of a child, the term refers specifically to the non-accidental commission of injuries against the child by or allowed by a parent(s)/guardian(s) or other person(s). The term also includes emotional, physical, severe physical, and sexual abuse as defined in CDSS MPP Section 31-002(c)(9)(D).
The CACI is a system that allows Children's Social Workers to access in written form to any child abuse records of individuals through the Department of Justice (DOJ) listing names and other identifying information compiled from child abuse reports submitted to DOJ by mandated child abuse reporting agencies which maintain information regarding allegations of abuse and/or neglect. This is primarily utilized to evaluate relative and nonrelative extended family members as prospective caregivers.
California’s version of the federal health care program called Early and Periodic Screening, Diagnosis and Treatment (EPSDT). It provides comprehensive medical, mental health and dental diagnostic and treatment services for all Medi-Cal eligible persons aged newborn to 21 years who request them. States are required to inform the families of eligible children about CHDP; assist with referral and transportation to providers; and, follow-up to ensure that necessary diagnostic and treatment services are provided.
Includes the intentional touching of the genitals or intimate parts or the clothing covering them, of a child, or of the perpetrator by a child, for purposes of sexual arousal or gratification. This does not include acts which are reasonably construed to be normal caretaker responsibilities, demonstrations of affection for the child, or acts performed for a valid medical purpose.
A general term for a device that can be installed in a vehicle and is designed to restrain, seat, or position children who weigh 50 pounds or less.
A group of individuals, as identified by the family, and convened by DCFS, who are engaged through a variety of team-based processes to identify the strengths and needs of the child or youth and his or her family, and to help achieve positive outcomes for safety, permanency, and well-being.
CFT Meetings are structured, guided discussions with the family, their natural supports and other team members. The meetings are designed to specifically address the family's strengths, worries that the family, agency or team members have regarding the child's safety, permanence and well-being. The family and team members develop a plan that builds on strengths, meets needs and considers the long-term views.
The term "child’s attorney" refers to the Children’s Law Center of Los Angeles (CLC) attorneys as well as the Los Angeles Dependency Lawyers (LADL) attorney appointed to represent the child in dependency proceedings. In addition, the term also refers to a paralegal, social worker or any other person working for that attorney. This also includes a youth’s delinquency attorney.
A non-profit corporation whose attorneys represent children in dependency court matters.
Support staff responsible for providing required notification to the child’s attorney, as detailed in a blanket minute order issued by the Presiding Judge of the Dependency court.
Collateral contacts are individuals or agencies with information that can assist the CSW in understanding the nature and extent of the alleged child abuse/neglect and in assessing the risk to and safety of the children. Collateral Contacts include professionals working with the child or parent and have regular contact with the family. Examples include: teachers, parole officers, physicians, DPSS, DMH, therapists, hospitals, and probation.
Sexual activity involving a minor under the age of eighteen (18) in exchange for something of value (i.e., food, shelter, money). [See PEN sections 11165.1(d)(2) and PEN 236.1(c)]. Exploitation includes instances when a minor exchanges sexual acts with a “John/date” even when there is no known trafficker/pimp; Examples of CSEC: Internet-based exploitation, pornography, stripping, erotic/nude massage, escort services, private parties, interfamilial pimping, child being exploited on the streets. CSE is a form of child abuse that mandated reporters must call in to the Child Protection Hotline for each new incident/episode. This includes reporting new AND repeated incidents of CSE on open cases.
The division within the California Department of Social Services (CDSS) responsible for licensing foster care facilities, i.e., foster family homes, foster family agencies, group homes and small family homes. Additional responsibilities include investigating any reported incident of child abuse, neglect or exploitation in such facilities and/or violations of licensing standards.
Offers counseling, nutrition classes, drug education and counseling, parenting classes, pre-natal care, continuing education, pre-employment training, family planning, group outings, and aerobic and weight training classes
Questions that may confuse a young child because they reference more than one response option. For example, 'Is it right or wrong to lie?'; 'Is your shirt green or yellow?'; 'Would your mom give you candy or punish you if you told a lie?'
Lowered resistance to infection.
Concurrent Planning aims to support timely permanence for children. Safe reunification is DCFS' first priority, but in the event that this is not possible, Concurrent Planning ensures that the identification of an alternative placement plan for children who cannot safely return home is in place from the beginning. Working with a labor/management group, the department implemented changes to Concurrent Planning which support the safety and permanence for children and families from the first day they enter out-of-home care. These system changes include focusing on identifying relatives and siblings and developing 'resource families' who are committed to working toward reunification and providing legal permanence if safe reunification is not successful. Concurrent Planning also engages families and draws on their strengths and uses ongoing assessments and case planning.
An assessment document as prescribed in Welfare and Institutions Code Sections 366.21(I), 366.22(b) and 361.5(g). The CPA is initiated by the case carrying Children's Social Worker and completed by the APRD CSW when adoption home study for attached children or matching/recruitment activities for unattached children are initiated.
Adoption petition was filed by the court and stamped with the filing and the action number.
Placement of a child six years and younger in a group home prior to the Disposition Hearing due to a special need for an in-depth evaluation that can only be completed in a "congregate care" facility. The placement cannot be more than 60 days unless and extension of the placement is included in the case plan and approved by the ARA. The child’s total time spent in the placement shall not exceed more than 120 calendar days.
When a party to a lawsuit needs to postpone a matter that has been calendared for a hearing or trial, the proper procedure is to apply to the court for a continuance (postponement to a later date).
CPM is a shared model of practice developed to better integrate services and supports for children, youth and families. The model emphasizes child-centered, family-based practice to identify strengths/needs, collaborative case planning and decision making that considers the long-term view for the family, and development of a support network (team) that will continue to be available to the family even after termination of formal services. The five key practice domains include Engaging, Teaming, Assessing, Planning & Intervening and Tracking.
An officer of the court who advocates the individual needs and best interests of a child, and provides the court with written recommendations. Persons serving as CASAs are generally community volunteers who participate in a training program, after which they are appointed as an officer of the court to advocate on behalf of a child(ren). CASAs are also referred to as Child Advocates or Guardians Ad Litem (GAL).
Refers to the parent with whom the child(ren) reside(s) (i.e., the parent with physical custody or primary physical custody).
Licensed clinician who provides assistance to CSW in identifying and assessing the needs of children with special needs by ensuring that the caregiver's home meets the child's needs and that all children having special needs have those needs met in accordance with the provisions of the Katie A. settlement agreement.
A deficiency is considered any failure to comply with any provision of the Community Care Facilities Act and/or regulations adopted by DCFS or the California Department of Social Services (CDSS) Community Care Licensing Division.
Developmental delay refers to infants and toddlers having a significant difference between the expected level of development for their age and their current level of functioning. (DCFS Glossary)
A disability that originates before an individual attains age 18 years, continues or can be expected to continue, indefinitely, and constitutes a substantial disability for that individual. The term includes mental retardation, cerebral palsy, epilepsy, and autism. It also includes disabling conditions found to be either closely related to mental retardation or to require treatment similar to that required for individuals with mental retardation, but shall not include other handicapping conditions that are solely physical in nature.
Services provided by the Regional Centers, which include diagnostic evaluation, coordination or resources such as education, health, welfare, rehabilitation and recreation for persons with developmental disabilities. Additional services include program planning, admission to and discharge from state hospitals, court-ordered evaluations and consultation to other agencies.
Involves a child who came to the United States for the purpose of adoption through the intercountry adoption process but entered foster care prior to finalization of the adoption regardless of the reason for the foster care placement. The disruption occurs after a child enters the United States under guardianship of the prospective adoptive parents or an adoption agency with a visa for the purposes of completing the adoption process domestically. The disruption must be reported even if the child's plan is reunification with the prospective adoptive parents and the stay in foster care is brief.
Family Code Section 297 defines domestic partners as two adults who have chosen to share one another’s lives in an intimate and committed relationship of mutual caring.
Welfare and Institutions Code Section 18291 (a) states that 'Domestic violence' means abuse committed against an adult or minor who is a spouse, former spouse, cohabitant, former cohabitant, or person with whom the suspect has had a child or is having or has had a dating or engagement relationship. Penal Code Section 13700 (b) states that "Domestic violence" means abuse committed against an adult or a minor who is a spouse, former spouse, cohabitant, former cohabitant, or person with whom the suspect has had a child or is having or has had a dating or engagement relationship. For purposes of this subdivision, "cohabitant" means two unrelated adult persons living together for a substantial period of time, resulting in some permanency of relationship. Factors that may determine whether persons are cohabiting include, but are not limited to, (1) sexual relations between the parties while sharing the same living quarters, (2) sharing of income or expenses, (3) joint use or ownership of property, (4) whether the parties hold themselves out as husband and wife, (5) the continuity of the relationship, and (6) the length of the relationship.
A child who is receiving AFDC- FC, Kin-GAP or AAP benefits and is concurrently a consumer of Regional Center services.
A web-based system used by the DHS Medical Hubs that tracks the health status of children in the child welfare system and facilitates provision of quality medical care. As part of a joint effort between DHS and DCFS, the E-mHub System accepts the electronic transmission of the DCFS Medical Hub Referral Form and returns appointment status alerts and completed examination forms, to DCFS via an e-mail notification. DCFS and DPH PHNs and PHN Supervisors have access rights to EmHub screens pertaining to the health care of children served at the Hubs. Completed examination forms may be accessed through the link in the email notification by using the SITE User ID (employee number) and Password (current password used by employee).
The EX Pass TAP Card/Sticker is a monthly pass good for MTA and local travel on twenty-four (24) different public transit carriers throughout the Greater Los Angeles region. No transfers are necessary between the EZ Pass TAP Card transit carriers.
Are characterized by severe disturbances in eating behavior. Eating disorders are divided into three categories: Anorexia Nervosa, Bulimia Nervosa, and Binge Eating.
Often seen in families where children are forced or allowed to work under certain illegal conditions outside and inside the home. This form of exploitation prohibits children from attending school and may place them in work environments that are a threat to their general health, safety and security. Although poverty may be a prime motivation for this type of exploitation, other situations may exist.
A stipend available to supplement (not replace) ILP. To qualify for this stipend, a youth must be eligible for ILP, be 18 years of age or older, and whose financial need has been verified by YDS. Current and former foster youth, as well as, Nonminor Dependents may qualify. The stipend may provide for, but not be limited to the following independent living needs: bus passes/transportation, housing rental and utility deposits and fees, education and work-related equipment and supplies, training-related equipment and supplies, auto insurance and driver’s education.
Emancipation allows a youth to be freed from the custody and control of their parents and to have many of the rights and responsibilities of an adult. There are three ways a minor may become emancipated: Get married with parental consent and permission from the court; Join the military; Go to court and have the judge declare you emancipated.
An ex-prate temporary restraining order issued by the Superior Court following a determination by law enforcement that a child is in immediate danger of abuse by a member of a child’s family or household. An EPO may exclude any parent, guardian or member of a child’s household from the dwelling of the person having the care, custody, and control of the child. EPO allow children to remain in their home while allegations of child abuse by the restrained parties are investigated and allow the non-offending parent time to seek assistance from Family Law Court. EPO expire at the close of the second day of judicial business following the day of issuance. EPO may only be extended by application to the appropriate court. See "Ex-Prate Order," "Judicial Business Hours" and "Restraining Order."
The term 'assessment' goes beyond the concept to evaluate a child's safety and risk, and to determine whether and what services are needed to ameliorate or prevent child abuse and neglect. In order to complete a thorough family assessment, any and all safety threats (as listed on the SDM Safety Assessment) that may compromise a child's safety and well-being must be thoroughly assessed, even if those safety threats were not identified on the referral as an allegation.
The term 'investigation' encompasses the efforts of DCFS to determine if abuse or neglect has occurred, if allegations can be substantiated.
"Emotional abuse" refers to nonphysical mistreatment, the results of which may be characterized by disturbed behavior on the part of the child such as severe withdrawal, regression, bizarre behavior, hyperactivity, or dangerous acting-out behavior.
CSW has good cause to request a ruling the same day the request is submitted, and intends to serve the warrant or at least make an attempt the same day it is granted.
Forcing or coercing a child into performing functions which are beyond his/her capabilities or capacities, or into illegal or degrading acts. The term also includes sexual exploitation, economic exploitation, exploitation involving illegal activities and exploitation in the home.
When assessing families that are involved in the gang culture investigate to see if children are encouraged from a young age to value gang membership (parents may be active or retired gang members), or if someone is teaching children gang signs, dress codes and affiliations and advocating membership, if adults are supporting violent behavior and criminal activities of the children.
Exploitation exists within the family household as well. A child may be selected to perform all or the majority of such parental tasks as cleaning, cooking and caring for younger siblings, including bathing, dressing, feeding and babysitting. Frequently, the child who is singled out in this manner is substituting for a parent who is absent or unable to fulfill parental responsibilities due to the parents' substance abuse and/or physical/mental disabilities.
The Extended Foster Care program allows a foster youth to remain in foster care and continue to receive foster care payment benefits (AFDC-FC payments) and services beyond age 18, as long as the foster youth is meeting participation requirements, living in an approved or licensed facility, and meeting other eligibility requirements.
A method of bringing family members together to come up with a recommendation to the court for a safe and permanent plan for a child. If differs from the traditional child welfare case conferencing in that although the caseworker participates in an information-sharing capacity, the family and not the child welfare worker is "in charge" of the meeting and responsible to create the recommended plan. Refer to the memo dated 1/12/15 from the DCFS Chief Deputy Director, "Teaming with Families - Operational Guidelines for Moving From Team Decision Making Meetings to Child and Family Teams" located in the Director’s Page under Memos from the Chief Deputy Director and the CPM website.
In January 1991 as a result of Senate Bill AB546, we established comprehensive community-based networks and services to protect children while they remain within their homes. The primary goal of the Family Preservation approach is the safety of children in their own homes and safe return of children being reunified after periods of placement into foster care. DCFS currently works with 38 Family Preservation agencies and covers most of Los Angeles County. On average, 5,000 families are served annually. The maximum length of time services can be provided is 12 months. The average stay in Family Preservation is 9 months.
Activities designed to provide time-limited foster care services to prevent or remedy neglect, abuse, or exploitation. The child remains in temporary foster care while services are provided to reunite the family.
An on-line Structured Decision Making (SDM) tool used for identifying family strengths and needs and to assist with case planning.
The term 'first degree relative' refers to grandparents, uncles, aunts, and adult siblings.
The Foster Care Search Engine (FCSE) is a web-based system providing an interactive search mechanism using Geographic Information System (GIS) technology. The system is a tool used to identify vacant placement homes within Los Angeles County based on the children needs and well-being. Mapping capability allows for staff to view location of vacancies in proximity to schools, community boundaries and placement of siblings. The system interfaces with CSW/CMS Datamart database to maintain data integrity and provides a web-based data entry screen for Foster Family Agencies to provide specific data not available on CWS/CMS. The system is used by Children’s Social Workers (CSW) and by Technical Assistants (TA) who assists the workers in foster care placements.
A non-profit organization licensed by the State of California to recruit, certify, train, and provide professional support to foster parents.
Greater Avenues for Independence - CalWORKs services may include GAIN services (Welfare-to-Work Program). GAIN is mandatory for parents aided on CalWORKs, unless there is an exemption (e.g., parent has a child under a year old, temporary incapacity, participant is over age 65).
A portion of the cash aid being received by a CalWORKs participant is reduced when (s)he is not adhering to GAIN Program requirements.
Penal Code Section 11165.2(b) defines general neglect as the negligent failure of a person having the care or custody of a child to provide adequate food, clothing, shelter, medical care, or supervision where no physical injury to the child has occurred.
The unavailability of a preferred placement, after a diligent search has been conducted; or the desires of the Indian parent, child, or tribe; or the child’s special needs for a placement, which offers either proximity to a parent or a therapeutic program when no available preferred placement can meet these needs.
For the purpose of the adoption home study, procedures initiated on behalf of the applicant, at the applicant's request, to appeal the Department's decision when the adoption home study has been denied by DCFS. The Grievance Review Process pamphlet outlines the specific action taken by the Department when the applicant requests a grievance review hearing. In addition, grievance procedures are in place for foster parents who want to challenge the Department's decision in regards to their care and supervision of a child(ren). Foster parents who want to challenge decisions regarding their license must follow grievance procedures from the State Department of Social Services.
Refers to behaviors or factors that may increase the risk of contracting HIV/AIDS such as: sexual activities involving exposure to the blood or semen of an infected person, sharing needles used for intravenous (IV) injections, tattooing and body-piercing with infected persons, maternal transmission (i.e., from an infected mother to her fetus during pregnancy, birth or breast feeding) when the infant’s parent has a history of behavior that places the parent at an increased risk of exposure to HIV, blood or blood products, transfusions or organ transplants during the period from 1978 to June of 1985, and child is a victim of sexual abuse that places them at risk of exposure to HIV.
Harassment is unlawful violence, a credible threat of violence, or a knowing and willful course of conduct directed at a specific person that seriously alarms, annoys, or harasses the person, and that serves no legitimate purpose. The course of conduct must be such as would cause a reasonable person to suffer substantial emotional distress, and must actually cause substantial emotional distress to the petitioner. (California Code of Civil Procedure Section 527.6 (a)(3))
An individual designated to make medical decisions on behalf of an adult if (s)he is incapable of making her/his own health care decisions. If no health care agent is appointed, when an adult has a medical emergency in which (s)he is not capable of communicating with hospital staff, the parent(s) or other relative would be asked to make decisions about medical treatment for the individual.
Passed in 2003, the Health Insurance Portability and Accountability Act (HIPAA) is designed to give patients more control over their health information, set boundaries on the use and disclosure of health information, institute safeguards to protect privacy of health information, create accountability, civil and criminal penalties, and establish a balance between individual privacy and the public good. In cases where the law of California is more restrictive than HIPAA, the State law must be followed. Conversely, if HIPAA is more restrictive than State law, then HIPAA must be followed unless there is a legal exception.
A document that is generated on CWS/CMS that contains a summary of a child's health and education information. The caregiver keeps a current copy of the Passport, along with the health and education forms in a binder provided by DCFS. This binder shall follow the child to all placements. The Passport shall accompany the child to all medical, dental and educational appointments. The Passport binder in its entirety is given to the child upon emancipation.
A plan developed by a medical provider that assists the child/youth in developing life long practices that encourages healthy behaviors, healthy food choices and regular engagement in cardio-vascular activities.
In the context of CHDP, a child with one or more of the following conditions: A past significant medical problem or chronic illness; possible contagious disease; medication; and/or social problems (e.g., language barrier) which could conceal an unmet medical need.
The county that provides courtesy supervision for a child residing with a relative or in foster care placement whose legal jurisdiction is in another California County.
An approach to successfully connect individuals and families experiencing homelessness or housing instability to housing services without preconditions and barriers to entry such as service participation requirements.
The DCFS ICPC Unit will contact the potential host state, per existing procedures and obtain information regarding provision of services to a NMD placed in a SILP.
Shortcomings that if not corrected would have direct and immediate risk to health, safety, or personal rights of the child.
There is reasonable cause to believe that the child will experience serious bodily injury in the time it would take for the CSW to return to the office, prepare, obtain from a judge, and serve the removal order.
A report determined by the investigator conducting the investigation not to be unfounded, but the findings are inconclusive and there is insufficient evidence to determine whether child abuse or neglect, as defined in Section 11165.6, has occurred.
The adoption of a child in which neither CDSS nor an agency licensed by CDSS, such as DCFS, is a party to, or joins in, the petition for adoption.
The Lanterman Developmental Disabilities Act requires that a person who receives services from a regional center have an Individual Program Plan (IPP). Person-centered individual program planning assists persons with developmental disabilities and their families to build their capacities and capabilities. The planning team decides what needs to be done, by whom, when, and how, if the individual is to begin (or continue) working toward the preferred future. The document known as the Individual Program Plan (IPP) is a record of the decisions made by the planning team.
Those individuals who develop a health care plan for a child with special health care needs in a specialized foster care home or group home which shall include the child's primary care physician or other health care professional designated by the physician, any involved medical team, and the CSW and any health care professional designated to monitor the child's individualized health care plan, including, if the child is in a certified home, the registered nurse employed by or under contract with the certifying agency to supervise and monitor the child. The child's individualized health care plan team may also include, but shall not be limited to, a public health nurse, representatives from the California Children's Services Program or the Child Health and Disability Prevention Program, regional centers, the county mental health department, and where reunification is the goal, the parent or parents, if available. In addition, if the child is in a specialized foster care home, the individualized health care plan team may include the prospective specialized foster parents, who shall not participate in any team decision.
A person is considered institutionalized when (s)he has been residing in a hospital, jail, prison, homeless shelter, residential school, rehabilitation center, halfway house, out-of-home care facility, etc., for more than 90 calendar days. This does not include battered women's shelters.
ISWs are the key component when detention is being considered or when a detention has occurred. ISWs provide immediate linkage to services for families where a court detention was necessary. ISWs participate in child safety conferences shortly after detention to review for possible return of children and or to connect children and families to services immediately following detention.
The Intensive Treatment Foster Care Program (ITFC) was developed to meet the treatment needs of emotionally disturbed children who need out-of-home placement. An Intensive Treatment Foster Care agency refers to an organization licensed by the California Department of Social Services for children who have a history of emotional/behavioral disturbance, have experienced multiple placement histories; are at risk of hospitalization, and/or qualify for Rate Classification Level (RCL) 12 or higher group home placement.
One agency has custody of the child and another agency approved the applicant assessment.
A hearing that is not mandated by the Welfare and Institutions Code, but is set by the court to address specific information and/or receive a progress report on the case at hand.
The computer system tracking all dependency court schedules and proceedings. Additionally, this software system allows DCFS to print minute orders.
The intent of the Kin-GAP program is to establish a program of financial assistance for relative caregivers who have legal guardianship of a child while Dependency Court jurisdiction and the DCFS case are terminated. The rate for the Kin-GAP program will be applied uniformly statewide.
The Kinship Support Division promotes, increases, and sustains legal permanency for children, adolescents and young adults in relative and legal guardianship placement through providing education, supportive services, advocacy, mentoring, and aftercare that is accessible and meets the needs of the child, family, and community.
Physical custody of a minor 72 hours old or younger accepted by a person from a parent of the minor, who the person believes in good faith is the parent of the minor, with the specific intent and promise of effecting the safe surrender of the child.
Questions that suggest a desired answer; often these are questions that can be answered with a simple 'yes' or 'no.' For example: "The sky is blue, isn't it?"
Legal relief (legal remedy): the means to achieve justice in any matter in which legal rights are involved. Remedies may be ordered by the court, granted by judgment after trial or hearing, by agreement (settlement) between the person claiming harm and the person he/she believes has caused it, and by the automatic operation of law. Some remedies require that certain acts be performed or prohibited (originally called "equity"), others involve payment of money to cover loss due to injury or breach of contract, and still others require a court's declaration of the rights of the parties and an order to honor them.
Involves a child who was previously adopted from overseas (whether the full and final adoption occurred in the foreign country or domestically) but entered foster care as a result of a court terminating the parents' rights or the parents' relinquishing their rights to the child.
A child whose birth parents have had his or her parental rights terminated or whose birth parents have voluntarily given up parental rights through relinquishment.
Includes the intentional masturbation of the perpetrator's genitals in the presence of a child.
Foster family homes, small family homes, group homes, foster family agency certified homes, child care facilities.
Any medical procedure or intervention that will serve only to prolong a state of unconsciousness where there is a reasonable degree of medical authority that such state of unconsciousness is permanent, or prolong a terminal condition."
A criminal history check based upon the submission of the subjects' fingerprints to the DOJ. The inquiry may also include an inquiry of the Child Abuse Central Index and an inquiry of the FBI database, if there is an indication that the subject may have been arrested outside of California, or that the subject has been a resident of California for less than two years. The clearance will confirm the identity of the subject of the inquiry and give the subject's history of arrests and convictions.
Degree to which there are stated, shared and understood safety, well-being, and permanency outcomes and functional life goals for the child and family. The outcomes and goals should outline required protective capacities, desired behavior changes, sustainable supports, and other accomplishments necessary for the child and family to achieve and sustain adequate daily functioning and greater self-sufficiency.
California's federal Medicaid program.
As defined by Civil Code (CIV) Section 56.05(g), is any individually identifiable information, in electronic or physical form, in possession of or derived from a provider of health care, health care service plan, pharmaceutical company, or contractor regarding a patient’s medical history, mental or physical condition, or treatment. This does not include psychotherapy notes (notes made by the therapist about a private therapy session that are kept separate from the rest of the patient’s medical record). These notes are subject to additional privacy protections and cannot be disclosed by therapists even in situations where other PHI may be disclosed.
One or more of the following exist: Previous significant medical problem or chronic illness; possible contagious disease; on medication; and/or, social problem or language barrier which could conceal an unmet medical need.
Children with special health care needs as defined by Assembly Bill 2268. These children have medical conditions and symptoms that require special procedures, may be temporarily or permanently dependent upon medical equipment and/or devices, therapies and may require ongoing medical care and assessment as determined by the child’s physician. The caregiver must have been trained to provide the specialized in-home health care to these children.
A motion for rehearing or reconsideration: seeking to alter or amend a judgment or order.
For youth whose behavior places them at risk of entry into the juvenile justice system, particularly those who are subject of a 241.1 assessment. The goal of the therapy is to improve caregiver discipline practices, enhance family relations, decrease youth association with deviant peers, increase pro-social peers, improve youth school or vocational performance, engage youth in pro-social recreational outlets, and develop a support network of extended family, neighbors, and friends to help achieve and maintain such changes. (Only available in Regional Offices in SPA 6 and 7)
A program which provides a comprehensive, multi-level intervention to children and youth in the child welfare system. MTFC is an evidence-based practice (EBP). MTFC Program provides each youth with short-term treatment (average 6-12 months) in specialized foster home environment where child/youth is the only foster child and has the following: own bedroom, an individual therapist, a skills trainer, attend public school, foster parents trained in the MTFC model, permanent caregivers receive behavior training and family therapy before and after the youth is returned to their home, a program supervisor that coordinates all care and is available 24/7.
The cornerstone of and entry point to the Protective Services Child Health (PSCH) system and the focal point for a community-based Provider Network. The KDMC Hub will provide timely, comprehensive medical, developmental and psychological assessments, as well as on-site preventive health services to children in out-of-home care. In addition, the Hub will assist in the development of a comprehensive child health plan for each child, provide referrals for follow-up care and conduct provider outreach. (DCFS Glossary, from "Hub Services: King/Drew Medical Center (KDMC)")
Any team of three or more people trained in the prevention, identification, management or treatment of child abuse or neglect cases and qualified to provide a broad range of services related to child abuse or neglect. The team may include a CalWORKs case manager, whose primary responsibility is to provide cross program case planning and coordination of CalWORKs child welfare services of those mutual cases or families that may be eligible for CalWORKs services and that, with the informed written consent of the family, receive cross program case planning and coordination.
A near fatality is a severe injury or condition caused by abuse or neglect that results in the child receiving critical care for at least 24 hours following admission to a critical care unit.
The failure to provide a person with necessary care and protection. In the case of a child, the term refers to the failure of a parent(s)/guardian(s) or caretaker(s) to provide the care and protection necessary for the child's healthy growth and development. Neglect occurs when children are physically or psychologically endangered. The term includes both severe and general neglect as defined by Penal Code Section 11165.2 and medically neglected infants as described in 45 Code of Federal Regulations (CFR) Part 1340.15(b).
A network (also known as a support network, support system, or social support system) refers to an extended group of family, friends, neighbors, professionals, and/or cultural, religious, or other communities that provide support for -- and meet a wide range of needs for -- a parent/caregiver and/or the child/ren (including tribal ICWA programs, Indian organizations, and/or family members, which can include non-related tribal members). The network may consist of individuals or organizations (e.g., religious organizations, community organizations, professional providers) who care about the child/ren or family and who provide or share concrete support (e.g., financial help, transportation, babysitting) or emotional support (e.g., listening, advice).
Children who first, or initially, enter the child welfare system and are placed in out-of-home care under a WIC 300 petition. (This definition includes children in an open case under a Court FM or VFM case plan who are subsequently removed from their biological parents and placed in out-of-home care).
A hearing in which the affiliated parties are not required to appear in order for the court to proceed with the matter at hand.
Non-Child Welfare Department module within CWS/CMS used to enter non-court cases such as Kin-GAP. It contains placement and payment information, the Legal Guardian’s information and case notes. The Probation Department also enters information in the Non-CWD module for cases supervised by their department.
A relative other than the child's birth or adoptive parents.
A person appointed by the Superior Court pursuant to the provisions of the Probate Code or appointed by the Dependency Court pursuant to the provisions of the Welfare and Institutions Code, who does not meet the definition of a 'Related Legal Guardian.'
A hospital, jail, prison, homeless shelter, residential school, rehabilitation center, halfway house, out-of-home care facility, etc. where the individual has lived for more than 90 calendar days. This does not include battered women's shelters.
A current dependent child or ward of the juvenile court, or a nonminor under the transition jurisdiction of the juvenile court, who: has attained 18 years of age while under an order of foster care placement by the juvenile court; is in foster care under the placement and care responsibility of the county welfare department, county probation department, Indian tribe, consortium of tribes, or tribal organization; is participating in a transitional independent living case. Defined by WIC 11400(v).
A nonrelative extended family member is defined as an adult caregiver who has an established familial relationship with a relative of the child or a familial or mentoring relationship with the child. The county welfare department must verify the existence of a relationship through interviews with the parent and child or with one or more third parties.
Includes any sexual contact between the genitals or anal opening of one person and the mouth or tongue of another person.
also known as intravenous feeding, is a method of getting nutrition into the body through the veins. While it is most commonly referred to as total parenteral nutrition (TPN), some patients need to get only certain types of nutrients intravenously.
DPSS term for person receiving services.
This is a six-week, 33-hour program that prepares resource families (foster and adoptive) for the new roles and parenting skills they will need if they adopt. A program of mutual preparation and selection which uses the teamwork approach between foster and adoptive parents and the agency to prepare foster and adoptive parents for theexperience of parenting children with special needs, such as those supervised by DCFS. The program incorporates self-assessment, mutual decision-making and experiential preparation for foster and adoptive planning to help parents decide if their expectations and abilities match the realities of foster and adoptive parenthood.
An economic loss or expense resulting from an injury or death to a victim of crime that has not been and will not be reimbursed from any other source. This is related to compensation from being a Victim of Crime.
Includes any intrusion by one person into the genitals or anal opening of another person, including the use of any object, except for acts performed for a valid medical purpose.
Includes any of the following options: the child returns home, the court approves adoption, legal guardianship, permanent plan living arrangement with a relative/non-relative extended family member, or the child's case is closed.
The services provided to achieve legal permanence for a child when efforts to reunify have failed until the court terminates FR. These services include identifying permanency alternatives, e.g., adoption, legal guardianship, tribal customary adoption and planned permanent living arrangement. Depending on the identified plan, the following activities may be provided: inform parents about adoptive planning and relinquishment, locate potential relative caregivers and provide them with information about permanent plans (e.g., adoption, legal guardianship) and refer the caregiver to the Adoption Division for an adoptive home study, etc.
Permanency Planning Conferences (PPCs) are modeled after TDM meetings to ensure that a multi-disciplinary team of professionals, family members and caregivers meet regularly to focus on the urgent permanency needs of youth. Refer to the memo dated 1/12/15 from the DCFS Chief Deputy Director, "Teaming with Families - Operational Guidelines for Moving From Team Decision Making Meetings to Child and Family Teams" located in the Director’s Page under Memos from the Chief Deputy Director and the CPM website.
In the context of adoption, substantially correct information regarding a prospective adoptive parent. This shall include, but is not limited to, the following: full legal name; age; religion; race or ethnicity; length of current marriage and number of previous marriages; employment; whether other children or adults reside in the home; whether there are other children who do not reside in the home and the child support obligation for these children and any failure to meet these obligations; any health conditions curtailing normal daily activities or reducing normal life expectancies; any convictions for crimes other than minor traffic violations; any removal of children due to child abuse or neglect; and, general area of residence, or upon request, address.
Pertinent collateral contacts are individuals or agencies with information that can assist the CSW in understanding the nature and extent of the alleged child abuse/neglect and in assessing the risk to and safety of the children. Collateral Contacts include professionals working with the child or parent and have regular contact with the family. Examples include: teachers, parole officers, physicians, DPSS, DMH, therapists, hospitals, and probation.
Non-accidental bodily injury that has been or is being willfully inflicted on a child. It includes willful harming or injuring of a child or endangering of the person or health of a child defined as a situation where any person willfully causes or permits any child to suffer, or inflicts thereon, unjustifiable physical pain or mental suffering, or having the care or custody of any child, willfully causes or permits the person or health of the child to be placed in a situation such that his or her person or health is endangered.
Shortcomings that without correction would become a risk to the health, safety, or personal rights of the child. The child can be placed in the home pending completion of the CAP. TANF/CalWORKs is the funding source possibly available to the caregiver until the CAP is completed and eligibility for federal Foster Care funding is determined.
A meeting of attorneys and parties held for the purpose of reaching a negotiated settlement involving joint solutions.
A PPT is held for any pregnant or parenting teen under the Department’s supervision (as well as potential and recent fathers) as a youth-centered approach in order to identify and discuss issues related to pregnancy and early stages of child-rearing as well as breaking intergenerational cycles. Refer to the memo dated 1/12/15 from the DCFS Chief Deputy Director, "Teaming with Families - Operational Guidelines for Moving From Team Decision Making Meetings to Child and Family Teams" located in the Director’s Page under Memos from the Chief Deputy Director and the CPM website.
Provides for 12 months in a residential program and a 12-month outpatient transitional services program.
i.e., more likely than not
A man is presumed to be the biological father of a child if: He has signed a voluntary declaration of paternity (VDP) or, after January 1, 1997 is identified on the child’s birth certificate; He and the mother are or have been married to each other and the child is born during the marriage or within 300 days after the marriage is terminated; Before the child’s birth, he and the child’s birth mother have attempted to marry each other and the child was born during the attempted marriage or within 300 days after the termination of cohabitation; After the child’s birth, he and the child’s birth mother have married or attempted to marry and either with his consent he is named on the child’s birth certificate or he is obligated to pay child support; He receives the child into his home and openly holds out the child as his birth child; Anyone whom a court has found to be a presumed or legal father (this includes family court, dependency court, and judgments for child support services);Other men who tried to marry the mother or thought they had married the mother (even if it turns out that they did not), and even if after the birth may qualify as a presumed father. Consult County Counsel.
As it pertains to the allegations in a child welfare case, the petition must include enough facts that if later proven, will cause a child to be declared a dependent of the court.
Reasonable cause or a reasonable ground for belief in certain alleged facts (more than a hunch, but less than absolute certainty).
As defined by Health Insurance Portability and Accountability Act (HIPAA), is health (including mental health) information created or maintained by a health care provider that identifies or can be used to identify a specific individual. PHI relates to an individual’s health, health care or payment for care – in the past, present or future.
Medications used as tools for producing certain chemical and physiological effects in the central nervous system. They are usually classified according to the types of disorders they are primarily used to treat.
A pro bono law office serving low-income children, adults, and families. Through its Children's Rights Project, Public Counsel assists children in civil legal matters such as guardianship, adoption, special education, government benefits, emancipation, teen parenting issues, immigration, mental health services, access to education and transitional services upon emancipation from foster care.
Referral Address Verification System
Includes any penetration however slight, of the vagina or anal opening of one person by the penis of another person, whether or not there is the emission of semen.
An intervention, informed by a Housing First approach, that connects families and individuals experiencing homelessness or housing instability to assistance that may include the use of time-limited financial assistance and targeted supportive services.
The law requires child welfare agencies to make reasonable efforts to provide services that will help families remedy the conditions that brought the child and family into the child welfare system. It is based upon a standard of reasonableness, which is a subjective test of what a reasonable person would do in the individual circumstance, taking all factors into account. This includes conducting a Due Diligence search to locate parents whose whereabouts are unknown.
When it is objectively reasonable for a person to entertain a suspicion, based upon facts that could cause a reasonable person in a like position, drawing when appropriate, on his or her training, to suspect child abuse or neglect.
The standard characterized by careful and sensible parental decisions that maintain the child's health, safety, and best interest.
The DCFS office that is responsible for providing services to the child, youth, dependent, or nonminor dependent. Usually, the office where the child's CSW is located.
Court will rule on the request by 5:00 p.m. the day after the request is filed with the court.
An adult who is related to the child by blood, adoption or affinity within the fifth degree of kinship, including stepparents, stepsiblings, and all relatives whose status is preceded by the words, 'great,' 'great-great' or 'grand' or the spouse of any of these persons even if the marriage was terminated by death or dissolution. A former stepparent is considered a relative only if the child is federally eligible.
For the purpose of placement and foster care payments: An adult who is related to the child by blood, adoption or affinity within the fifth degree of kinship, including stepparents, stepsiblings, and all relatives whose status is preceded by the words, "great," "great-great" or "grand" or the spouse of any of these persons even if the marriage was terminated by death or dissolution.
The action of a parent in which he or she surrenders custody, control and any responsibility for the care and support of the child. Currently, only an Adoption social worker or the court is qualified to process a relinquishment.
The RMP is a family centered, multi-departmental, integrated approach to identifying, coordinating and linking appropriate resources/services to meet the needs of children currently in, or at risk of a RCL 6 through 14 placement. Additional information can be found at www.lacdcfs.org/katieA/RMP/. Refer to the memo dated 1/12/15 from the DCFS Chief Deputy Director, "Teaming with Families - Operational Guidelines for Moving From Team Decision Making Meetings to Child and Family Teams" located in the Director’s Page under Memos from the Chief Deputy Director and the CPM website.
Families that have a foster care license and an approved family assessment that meets the State’s adoption standards. They are dually prepared to provide foster care and support family reunification; but, should reunification not occur, they are approved to provide an adoptive home for a child.
An order issued by the court, which enjoins a person from engaging in a specified behavior or activity, limits the distance a person may approach a specific location and/or person, or excludes a person from a specific dwelling or place of business. See "Emergency Protective Order."
For children aged three or older at the time of initial removal, services are to be provided from the dispositional hearing until the 366.21(f) hearing, unless the child is returned home. For children under the age of three, services are to be provided until the 366.21(e) hearing, unless the child is returned home.
The Review Agent conducts the Grievance Review Hearing. In accordance with CDSS Manual of Policies and Procedures (MPP) 31-020.511-.513, the Review Agent is a staff or other person not involved in the complaint; neither a co-worker nor a person directly in the chain of supervision of any of the persons involved in the complaint unless the Agent is the Director or Chief Deputy of the county; knowledgeable of the field and capable of objectively reviewing the complaint. The Review Agent for Los Angeles County, DCFS is the Manager, Appeals Section.
Supplemental Security Income. This program pays monthly benefits to blind or disabled children/youth who have limited income and resources. It is administered by Social Security.
Specialized Supportive Services - CalWORKs participants eligible to receive GAIN services may be eligible to receive Specialized Supportive Services (e.g., mental health, substance abuse, domestic violence assessment and treatment services) and transportation, child care and other ancillary expenses.
The D-Rate is the rate paid on behalf of hard-to-place children with severe and persistent emotional and/or behavioral problems. This rate can be paid for eligible children placed in the following types of out-of-home care facilities if they have been certified for the D-Rate: foster family homes, non-related legal guardian homes, nonrelative extended family member homes, foster care-eligible relative (Youakim) homes, and small family homes which are not vendorized by Regional Center but are licensed for mentally disordered/emotionally disturbed children.
The school that the foster child attended when permanently housed (prior to detention) or the school in which the foster child was last enrolled. If the school the child attended when permanently housed is different than from the school the child was last enrolled, or if there is some other school that the foster child attended with which he/she is connected (and attended within the immediately preceding 15 months) the local educational agency foster child education liaison, in consultation and agreement with the foster child and their Educational Rights Holder, can determine which school should be the child's school-of-origin.
Is defined as being able to meet one’s basic needs for food, shelter, income, and overall functioning. It is complementary to the goal of permanency, as individuals typically function better when they are surrounded by loving and caring adults. However, if one’s safety net were to be removed, self-sufficient adults would still be able to survive. In order for youth to become thriving, self-sufficient adults, they need to acquire solid assets and skills, early on, in key areas and outcome areas, such as, permanency/housing; education; social and emotional well-being; career/workforce readiness; health and medication. These four outcome areas lay the foundation for a successful transition into adulthood. To develop properly, they must be addressed and nurtured early on, at the first point of contact. Having continuous high expectations for success in these four areas is critical if youth are to have the support they need to achieve self sufficiency.
Reasonable cause to believe that the child has a need for medical care for a serious medical condition; or is in danger of physical or sexual abuse; or the physical environment poses a threat to the child's health or safety.
Penal Code Section 11165.2(a) defines severe neglect as the negligent failure of a person having the care or custody of a child to protect the child from severe malnutrition or medically diagnosed nonorganic failure to thrive. "Severe neglect" also means those situations of neglect where any person having the care or custody of a child willfully causes or permits the person or health of the child to be placed in a situation such that his or her person or health is endangered, as proscribed by Penal Code 11165.3, including the intentional failure to provide adequate food, clothing, shelter, or medical care. Child abandonment would come under this section.
Includes any single act of abuse which causes physical trauma of sufficient severity that, if left untreated, would cause permanent physical disfigurement, permanent physical disability, or death; any single act of sexual abuse which causes significant bleeding, deep bruising, or significant external or internal swelling; or repeated acts of physical abuse, each of which causes bleeding, deep bruising, significant external or internal swelling, bone fracture, or unconsciousness.
The victimization of a child by sexual activities, including, but not limited to, those activities defined in Penal Code Section 11165.1(a)(b)(c). See "sexual assault" and "sexual exploitation."
Conduct in violation of laws pertaining to: Section 261 (rape), 264.1 (rape in concert), 285 (incest), 286 (sodomy), subdivisions (a) and (b) of Section 288 (lewd or lascivious acts upon a child under 14 years of age), 288a (oral copulation), 289 (penetration of a genital or anal opening by a foreign object), or 647a (child molestation). If there are no indicators of abuse, “sexual assault” does not include voluntary sodomy, voluntary oral copulation, or voluntary sexual penetration unless the conduct is between a person 21 years of age or older and a minor under 16 years of age.
Conduct involving matter depicting a minor engaged in obscene acts in violation of Section 311.2 (preparing, selling, or distributing obscene matter) or subdivision (a) of Section 311.4 (employment of minor to perform obscene acts). Any person who knowingly promotes, aids or assists, employs, uses, persuades, induces or coerces a child, or any person responsible for a child's welfare who knowingly permits or encourages a child to engage in, or assist others to engage in, prostitution or a live performance involving obscene sexual conduct or to either pose or model alone or with others for the purpose of preparing a film, photograph, negative, slide, drawing, painting or other pictorial depiction involving obscene sexual conduct. 'Person responsible for a child's welfare' means a parent, guardian, foster parent, or a licensed administrator, or employee of a public or private residential home, residential school, or other residential institution. Any person who depicts a child in, or who knowingly develops, duplicates, prints, or exchanges, any film, photograph, video tape, negative, or slide in which a child is engaged in an act of obscene, sexual conduct, except for those activities by law enforcement and prosecution agencies and other persons described in subdivisions (c) and (e) of Section 311.3.'
Sexually Transmitted Infections, including HIV and AIDS, are transmitted from one person to another through sexual contact as well as though direct person-to-person contact with blood or body fluids that contain the infection.
A sibling is defined as a child related to another person by blood, adoption, or affinity through a common legal or biological parent.
The determination of what is considered 'significant contact' by an individual with a child will be determined by the ASFA Division in consultation with County Counsel and regional staff.
Any residential facility in the licensee's family residence, which provides 24-hour care for six or fewer foster children who have mental disorders or developmental or physical disabilities and who require special care and supervision as a result of their disabilities. WIC 11400(e)
Assembly Bill 2268, defines children with special health care needs as those children who are either temporarily or permanently dependent upon medical equipment or in need of other specific kinds of specialized in-home health care, as determined by the child’s physician. See "medically fragile."
Definition for Adoption Assistance Program (AAP), a child whose adoption, without financial assistance, would be unlikely due to one or more of the following factors: age (three years or older),ethnic background, race, color or language, mental, physical, emotional or medical handicap, adverse parental background, membership in a sibling group which should remain intact. In the context of protective services childcare, a child who is mentally or physically incapable of caring for him/herself, as verified by a physician or a licensed or certified psychologist, and requires separate accommodations to be provided with basic childcare. In the context of dependency court, a special needs child is one who has had three or more placements during a 12-month period and has a diagnosis or history of one or more of the following: conduct disorder with aggressive tendencies or antisocial behavior; attention deficit disorder treated by psychotropic drugs; self-destructive or suicidal behavior; use of psychotropic drugs; developmental disability; fire setting; manifestation of psychotic symptoms; somatizing or chronic depression or social isolation; severe sexual acting-out behavior and/or; substance abuse.
A rate paid in addition to the basic care rate for the care of children/youth with special needs.
Any of the following foster homes where the foster parents reside in the home and have been trained to provide specialized in-home health care to foster children: 1) Licensed foster family homes; 2) small family homes or; 3) certified family homes that have accepted placement of a child with special health care needs who is under the supervision and monitoring of a registered nurse employed by, or on contract with, the certifying agency, and who is either of the following: a) a dependent of the court under WIC 300 or; b) developmentally disabled and receiving services and case management from a regional center.
Includes, but is not limited to, those services identified by the child's primary physician as appropriately administered in the home of any of the following: 1) A foster parent trained by health care professionals where the child is being placed in, or is currently in, a specialized foster care home; 2) Group home staff trained by health care professionals pursuant to the discharge plan of the facility releasing the child where the child was placed in the home as of Nov. 1, 1993, and who is currently in the home; 3) a health care professional, where the child is placed in a group home after November 1, 1993. WIC 17710(h)
The act of temporarily stopping a judicial proceeding through the order of a court.
Assesses the child's present danger and the interventions currently needed to protect the child. Assesses whether any children are likely to be in immediate danger of serious harm/maltreatment and determines what interventions should be initiated or maintained to provide appropriate protection.
A thirty (30) day pass good for MTA travel only. Students must have an appropriate MTA ID Card to obtain the pass. Student Cardholders are provided with a Student TAP Card each month. There is no charge for the Card itself. Students can pick-up a photo-less Metro Student Dare ID Card (K-8 or 9-12) at participating schools or one of the four Metro Customer Centers.
Substance Abuse and Drug Testing Services are available to determine whether parents or caregivers’ abilities are impaired by the use of alcohol and drugs; if parents/caregivers need to be referred for alcohol/substance abuse treatment, and to monitor progress in treatment. Test results are used as part of the evaluation process to determine if children can remain safely in the home of their parents and caregivers, or if children can be safely returned to the care of their parents and caregivers.
A report determined by the investigator conducting the investigation to constitute child abuse or neglect, as defined in Section 11165.6, based upon evidence that makes it more likely than not that child abuse or neglect, as defined, occurred.
SILP is a supervised and approved placement that is part of the Extended Foster Care program. SILP is a flexible and the least restrictive placement setting. It can include: an apartment (alone or with roommates); shared living situations; room and board arrangements; room rented from a landlord, friend or relative, or former caregiver; or college dorms.
CWS/CMS services component for nonminor dependents (NMD) under which the required Extended Foster Care (EFC) participation criteria must be indicated.
SOC refers to a continuum of care for children and their families, which meets their mental, emotional, and behavioral needs. The program focuses on treatment for children and youth who are at risk of placement in either a group home or a more restrictive setting. An Inter- Agency Screening Committee comprised of representatives from DCFS, Department of Mental Health, the Probation Department, Special Education Local Planning Area, and local school districts, screens these type of cases. Services may include intensive in-home treatment, in-home support services, daily living skills, mental health services, crisis intervention, respite care, parent training, school intervention and therapeutic foster homes.
Refer to the memo dated 1/12/15 from the DCFS Chief Deputy Director, "Teaming with Families - Operational Guidelines for Moving From Team Decision Making Meetings to Child and Family Teams" located in the Director’s Page under Memos from the Chief Deputy Director and the CPM website.
The Transit Access Pass (TAP) Card is a monthly pass good for MTA travel only.
A process utilizing a multidisciplinary assessment and team approach in working with children and their families. Includes community-based social workers and other child and family service providers that assist the family in identifying local supports that could help reduce stresses and improve family life. Parents play a key role in identifying their needs and the supports that would be most helpful in addressing them. Refer to the memo dated 1/12/15 from the DCFS Chief Deputy Director, "Teaming with Families - Operational Guidelines for Moving From Team Decision Making Meetings to Child and Family Teams" located in the Director’s Page under Memos from the Chief Deputy Director and the CPM website.
The removal of a child from the home of a parent or legal guardian and placement or facilitation of placement of the child in the home of a non-offending parent, relative, foster caregiver; group home or institutional setting.Temporary custody also includes: placing hospital holds on children; situations in which the CSW interrupts an established Family Law Court custody or visitation orders when the CSW believes that if the order is carried out, the child would be placed in immediate risk of abuse, neglect or exploitation and the child is allowed to remain in the home of the non-offending parent; situations in which DCFS requests that law enforcement remove a child from the home of his or her parent/legal guardian and the CSW places the child with a relative or unrelated caregiver; and situations in which the child is living with a relative or an unrelated caregiver and all of the following conditions exist: child’s parent is asking for the child to be returned home, CSW believes that the return of the child to his or her parent would place the child at risk of abuse, neglect or exploitation, CSW does not allow the child to be returned to his or her parent; and, the child remains in the home of the relative or is placed in out-of-home care.
When a child is declared free from the care custody and control of his or her birth parents by court action.
A free legal services organization focused solely on protecting the rights of impoverished, abused and neglected children in Los Angeles County – children in foster care, children with educational disabilities, children who need healthcare or public benefits, and children in need of legal guardianship or adoption.
For the purposes of assigning Dependency Investigation tasks, a traditional residence is a house, an apartment, room(s) in a shared house or apartment, or another residence not included under the definition of non-traditional residence.
Hearing held by the receiving county court to determine if the case transfer request will be accepted.
Hearing held by the sending county court to determine the appropriateness of the transfer request. The court may order a case transferred to a different county during the Transfer-Out Hearing.
A home that has been licensed or approved by an Indian child’s tribe or a tribal organization designated by the Indian child’s tribe, for foster or adoptive placements of an Indian child using standards established by the tribe.
In the context of adoption, a person who has applied to adopt a child but has not been matched with an available child, and is therefore considered "unattached" to a particular child. An applicant for adoption who is not already linked with a specific child to adopt.
In the context of adoption, a child for whom adoption is the identified permanent plan but for whom no prospective adoptive parent has been identified.
A report determined by the investigator conducting the investigation to be false, inherently improbably, to involve an accidental injury, or not constituting child abuse or neglect as defined in Section 11165.6.
An aggressive, standardized approach to infection control which treats all human blood and certain body fluids as if they were known to contain blood-borne pathogens.The extension of blood and body fluid precautions to all patients. Under universal precautions, blood and certain body fluids of all patients are considered potentially infectious for human immunodeficiency virus (HIV), hepatitis B virus (HBV), and other bloodborne pathogens. (CDC)
Authorities, e.g. CSWs, law enforcement, etc, have reasonable evidence that a parent is abusive, cannot provide love and support to the child, or will in some significant way interfere with the examination.
The provision of non-court, time-limited protective services to families whose children are in potential danger of abuse, neglect, or exploitation when the children can safely remain in the home with DCFS services. In order to receive VFM services, the family must be willing to accept them and participate in corrective efforts to ensure that the child's protective needs are met. There is a six-month time limit for this service.
The foster care placement of a child by or with the participation of DCFS acting on behalf of CDSS, after the parent(s)/guardian(s) of the child have requested the assistance of DCFS and signed a voluntary placement agreement form.
A legal document filed by DCFS in juvenile dependency court alleging that a child is described under Welfare and Institution Code (WIC) 300.
A hearing will be held no later than 120 days from the date of the Permanency Review Hearing. The purpose of a WIC Section 366.26 hearing is to identify and implement a permanent plan for a dependent child of the court. The court will then make findings and orders in the following order of preference: permanently terminate the rights of the parent or parents and order that the child be placed for adoption; or, without permanently terminating parental rights, identify adoption as the goal and order that efforts be made to locate an appropriate adoptive family for the child within a period not to exceed 180 days; or, appoint a legal guardian and issue letters of guardianship; or, order that the child be placed in long-term foster care, subject to the periodic review of the court under WIC 366.3.
A request to submit a report to the court when a hearing is not calendared, but the matter requires immediate court attention. Walk-on hearings may be appearance or non-appearance matters.
The Welfare and Institutions Code (WIC) section that describes abuse, neglect, exploitation, and other endangerment situations and conditions whereby a child may be removed from the care and custody of parents or legal guardians and declared a dependent of the court under DCFS supervision.
W-Homes provide foster care to dependent teen parents and their non-dependent children, while assisting the teen parent’s to develop the skills they will need to provide a safe, stable and permanent home for their children. This is not a new licensing category. A W-Home can be a family home, approved relative caregiver or non-relative extended family member’s (NREFM) home, or the home of a non-related legal guardian whose guardianship was established pursuant to WIC Section 366.26 or 360.
A situation where any person willfully causes or permits any child to suffer, or inflicts thereon, unjustifiable physical pain or mental suffering or having the care or custody of any child, willfully causes or permits the person or health of the child to be placed in a situation such that his or her person or health is endangered.
These include concerns the family, team members or DCFS have related to the safety of the children/youth. The worries help the team identify what is important to ensure a safe and secure future for the children/youth.
Wraparound is a multi-agency initiative. The Wraparound approach is a family-centered, strengths-based, needs-driven planning and service delivery process. It advocates for family-professional partnership to ensure family voice, choice and ownership. Wraparound children and family teams benefits children by working with the family to ensure Permanency. Wraparound is funded through Title IV-E funds. The average length of involvement with the program is 8 months. The primary focus of the program is to keep children out of residential placements and maintain them safely in their family and community.
The practice of using flipchart pads and markers to write all brainstormed team responses to the agenda items during the CFT meeting. Examples of what is charted include: Family goal, non-negotiables, strengths, worries, needs and the plan for "what could go wrong".
Refers to the socially constructed roles, behaviors, activities, and attributes that a given society considers appropriate for boys and men or girls and women. These influence the ways that people act, interact, and feel about themselves. Gender is different from Sex in that Sex is assigned at birth.
an internal understanding of one’s own gender (e.g. a person’s internal sense of being male, female or something else). Therefore, a transgender person’s gender identity does not match the sex assigned to him or her at birth.
Ideas on what possible needs may be driving a person's behavior.
Matters related to the safety and well-being of the child(ren)/youth that cannot be changed at the present time (e.g. children cannot be supervised by anyone under the influence). Non-negotiables are focused on the "now" and should give the team ideas about the limits to planning and clarity on what cannot be compromised.
A continuous learning process in which you think about your practice, and consciously analyze your decision-making. It is an important tool in developing insight based on professional experiences, drawing on theory and relating it to practice.
A continuous process by which the "right people" for the child, youth and family have formed a CFT that meets, talks and plans together. The CFT has the skills, family knowledge and abilities, necessary to define the strengths and needs of the child and family, in order to organize effective services specific to their needs.
A need is what drives a behavior and what makes a behavior functional for the person. The child and/or youth's needs should be the focus of the teaming process to ensure their safety and well-being. Recognizing the individual and family needs is central to the family-engagement and planning process.
Degree to which the focus child(ren), parents (including the non-custodial parent), family members, and caregivers are active ongoing participants (e.g. having a significant role, voice, choice and influence) in shaping decisions made about child and family strengths and needs, goals, supports and services.